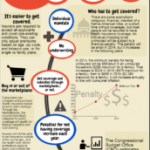
A quick overview of how individual health insurance will change in 2014 due to the Affordable Care Act (ACA).
Individual/Family Health

Health Insurance Premiums Coming To A W2 Near You
I’ve noted many times on this blog that one of the difficulties faced by proponents of health care reform is the fact that a lot of Americans are somewhat shielded from the actual cost of health insurance because a portion of their health insurance is paid for by their employer. And when we talk about… Read more about Health Insurance Premiums Coming To A W2 Near You

Pre-Existing Condition Insurance Plans (PCIP) Stop Accepting Applications
[…] Fortunately, Colorado has CoverColorado, which will continue to operate. But if you live in a state that has a federally-funded but state-run high risk pool and you need to secure coverage through it, make sure that you get your application submitted before March 2, 2013.
Looking beyond the PCIP, I have to wonder how this bodes for the health insurance exchanges/marketplaces and the entire individual health insurance market once plans are all guaranteed issue. The cost of caring for people with pre-existing conditions is high – there’s not really a way around that unless we can start making inroads into reducing the actual cost of care. And although guaranteed issue health insurance is definitely a step in the right direction in terms of getting access to healthcare for everyone, it’s also going to result in higher health insurance claims, and almost certainly higher health insurance premiums in the individual market. Hopefully the individual mandate will be successful at bringing enough young, healthy people into the insurance pool to offset the higher cost of care for people with expensive pre-existing conditions. With enough healthy people enrolled, the guaranteed issue individual market could be a solid health insurance pool. But if the balance shifts more towards unhealthy people, the individual market could start to resemble the structure of the PCIP, which isn’t sustainable in the long run without huge premium increases.
The ACAs Looming Premium Hikes are Big – How We Can Lower Them
It’s been almost three years since the ACA was signed into law, and in that time, the implementation process has been both steady and plagued with difficulties. The major provisions of the law have largely adhered to the original scheduled time frames, but there have been numerous hiccups along the way, culminating last summer in a Supreme Court case that challenged the legality of several aspects of the law. Once SCOTUS ruled in favor of the ACA, the path was largely cleared for implementation of the health insurance exchanges (marketplaces) that are scheduled to be open for business this fall with policies effective next January. The individual mandate will also take effect in January, but the penalty for not having health insurance in 2014 will be very small ($95 per uninsured person, or 1% of taxable household income). This has caused some concern that the mandate might not be strong enough to avoid the looming problem of adverse selection: specifically, that people who are in need of healthcare might be much more likely to purchase health insurance than people who are currently healthy once all plans are guaranteed issue.
Last month I wrote an article about how the ACA will largely erase the differences that currently exist between the small group and the individual health insurance markets. Once that happens, it would be odd to expect to not see a corresponding change reflected in the premiums. I think it’s unlikely that the premiums will equalize via a drop in small group premiums (if anything, the requirement that small group plan deductibles not exceed $2000 might mean that the average small group premiums increase too). The individual market is poised to become more like the small group market once the policies become guaranteed issue, and the premiums in the small group market are currently significantly higher than the premiums in the individual market. There will likely be a price decrease for people at the upper end of the age spectrum in the individual market, since their premiums are going to be limited to a maximum of 3 times the premiums for young people. But there is a growing concern that those young people – and probably a lot of people in the middle too – might be in for some sticker shock.
 Yes, the subsidies will help cushion the blow for people earning less than 400% of federal poverty level. But that still leaves a lot of people facing higher premiums and no subsidies. People who aren’t poor but definitely aren’t wealthy either – in other words, people who are middle class. Some of them are probably quite healthy. Some of them might have money stashed away in HSAs in order to pay for unexpected medical bills. Some of them might be happy to opt for higher deductibles and “catastrophic” health insurance plans in trade for lower premiums. But the way the ACA is currently written, they won’t be allowed to do that. The “catastrophic” plans will only be available to people under the age of 30 or people who meet the economic hardship qualifications. Everyone else will have to have at least a “bronze” plan that provides a broad range of benefits mandated by the ACA.
Yes, the subsidies will help cushion the blow for people earning less than 400% of federal poverty level. But that still leaves a lot of people facing higher premiums and no subsidies. People who aren’t poor but definitely aren’t wealthy either – in other words, people who are middle class. Some of them are probably quite healthy. Some of them might have money stashed away in HSAs in order to pay for unexpected medical bills. Some of them might be happy to opt for higher deductibles and “catastrophic” health insurance plans in trade for lower premiums. But the way the ACA is currently written, they won’t be allowed to do that. The “catastrophic” plans will only be available to people under the age of 30 or people who meet the economic hardship qualifications. Everyone else will have to have at least a “bronze” plan that provides a broad range of benefits mandated by the ACA.
Please don’t misunderstand me here. I firmly believe that our healthcare system needed […]
Patients Not Impressed By Recommendations For Less Preventive Care
Peggy Salvatore did an excellent job hosting the most recent Health Wonk Review – the Valentine’s Day Edition. I found this article by David Rothman, published at Health Affairs, to be particularly interesting. Although there has been much talk over the past few years about comparative effectiveness research, evidence-based medicine, and over-utilization of healthcare, patients… Read more about Patients Not Impressed By Recommendations For Less Preventive Care
The Downside Of Limited Benefit Association Health Plans
We recently worked with a client who is a Colorado REALTOR and a member of the National Association of REALTORS. She mentioned that she was eligible for coverage through NAR, but wanted to compare her options in the individual market with the policies that she could get as a NAR member. She sent over the details for us to look at, and we noticed that the coverage that NAR was touting as a benefit for members is basically just a guaranteed-issue limited benefit indemnity plan. Members have a choice of three different policy designs: The Physician Plan ($200/month for our client’s family of four) doesn’t include any inpatient benefits at all; it covers up to $100 per visit for office visits and ER visits, and up to $1000 for accidents. The Value Plan ($300/month for our client’s family) and Platinum Plan (almost $500/month) included limited inpatient and surgery benefits, but even the Platinum plan capped its benefits at $1000/day for inpatient care and $3000 per operating session for inpatient surgery. The plans are all guaranteed issue, but they have a 12 month pre-existing condition exclusion for any hospital or surgical expenses.
NAR makes it clear on their website – for people who are detail oriented – that the coverage offered through the REALTORS Core Health Insurance is not major medical and that the benefits are limited. They also provide a good informational page on their site about the struggles that self-employed people face when it comes to securing health insurance, and the efforts that NAR has made and continues to make in terms of making true group health insurance available to independent contractors who are part of a large association-type group like NAR. Presumably all of this will be a moot point as of next January when the individual mandate and guaranteed issue individual health insurance are implemented, but for now, it does appear that NAR is cognisant of the problems faced by many self-employed people who are trying to obtain medically-underwritten individual health insurance.
My concern is […]
Value Based Health Insurance Plan Design Pilot Program Shows Promise
[…] With HSA-qualified plans, there have long been concerns that policy-holders are more likely to avoid necessary as well as unnecessary treatments, in an effort to save money. This is because the plan structure usually doesn’t cover any costs except preventive care until the insured has met the deductible. With the sort of value-based plan design being tested in the San Luis Valley HMO program, care that has a high level of evidence-based backing might be covered with no cost-sharing, while other treatments require some financial contribution from the patient. So it’s not the same as an HSA-qualified plan’s structure that just relies on a high deductible to deter a patient from seeking excessive care. And instead of putting all of the burden on the patient, the value-based insurance design incorporates a team approach, with involvement from patients, doctors and health insurance carriers. All in all, it seems like an excellent idea.
It’s a Health Insurance Marketplace, Not An Exchange
HHS has officially started referring to “marketplaces” instead of “exchanges” when describing the state-based online venues where people will be able to purchase health insurance and receive income-based subsidies starting in 2014. Some are calling this a sign that HHS is desperate to garner approval for the ACA-created system for purchasing individual and small group… Read more about It’s a Health Insurance Marketplace, Not An Exchange
Strengthening The ACA Individual Mandate
Many people have expressed concerns that the mandate portion of the ACA isn’t strong enough to balance out the expected sharp increase in premiums that will accompany guaranteed issue coverage starting next year. Open enrollment windows are a possibility, but I’m not the only person who has noted that compressing each year’s applications into a… Read more about Strengthening The ACA Individual Mandate
Individual Health Insurance Premiums And The ACA
Chris Fleming hosted the Inauguration Edition of the Health Wonk Review this week at Health Affairs Blog, and it’s an excellent compilation of articles. The article written by one of our favorite bloggers, Maggie Mahar, about health insurance premiums in 2014 and beyond caught my attention, because that’s an issue we’ve been watching closely for some time. It’s a question that’s on a lot of minds right now – especially for people who buy their own health insurance and are in the segment of the population that is most likely to experience changes (in coverage, premium, how policies are purchased, etc.) in 2014. Jay and I not only work in the individual health insurance industry, but we’re also policyholders – we’ve have individual health insurance since 2003. We’ve had two carriers and several plan designs over the last decade, and we’ve experienced double digit percentage rate increases nearly every year (somewhat offset by the fact that we’ve been willing to increase our deductible and out-of-pocket limits several times).
We currently pay just over $400/month (for our family of four) for an Anthem Blue Cross Blue Shield CoreShare plan with a $3500 deductible and another $3500 in coinsurance. We know that our rate will go up in the fall – it always does – but how much? How much will prices go up for all of our clients who are covered by all of the biggest health insurance carriers in Colorado?
 I don’t know the answer to that question. And I don’t think that anyone really does. The post Maggie wrote references an article from Bob Laszewski that predicts rate increases of 25 – 50%, with some rates actually doubling, while Maggie’s prediction is more along the lines of a price decrease for people who qualify for subsidies, with an average price increase of just over 10% for those who don’t (anyone making more than 400% of FPL). The answers seem to change based on who’s doing the math, and it would be disingenuous to say that all of the numbers are objective. In general, I’ve found that the people who support the ACA are more likely to predict small rate increases and smooth sailing next year, while those who oppose the law are likely to predict large rate increases and general doom and gloom.
I don’t know the answer to that question. And I don’t think that anyone really does. The post Maggie wrote references an article from Bob Laszewski that predicts rate increases of 25 – 50%, with some rates actually doubling, while Maggie’s prediction is more along the lines of a price decrease for people who qualify for subsidies, with an average price increase of just over 10% for those who don’t (anyone making more than 400% of FPL). The answers seem to change based on who’s doing the math, and it would be disingenuous to say that all of the numbers are objective. In general, I’ve found that the people who support the ACA are more likely to predict small rate increases and smooth sailing next year, while those who oppose the law are likely to predict large rate increases and general doom and gloom.
Here’s what I do know.
The MLR (medical loss ratio) has already been in effect for two years. Carriers have had to limit their overhead to 15 – 20% of premiums since […]
Open Enrollment For Individual Health Insurance Plans Starting in 2014
Ever since the PPACA was first being discussed, the individual mandate has been touted as a buffer to protect health insurance carriers – and in turn, policyholders – from adverse selection that would otherwise certainly occur in a guaranteed issue individual market. It seemed that as long as people were required to maintain health insurance coverage, adverse selection would be minimized and people would be unlikely to purchase health insurance only during periods of sickness. But there was still enough concern about adverse selection that HHS issued a proposal for open enrollment periods in the individual market starting next year. This proposal was released at the end of November, and the specific details regarding the open enrollment period are on page 70595 of this Federal Register.
To sum it up, they’re proposing an initial open enrollment period for individual/family health insurance that starts in October 2013 and runs through the end of March, 2014 (a six month window in order to accommodate the large influx of initial applications), and then open enrollment periods that mirror Medicare’s: October 15th until December 7th each year. Beyond that window, only “qualifying event” applications would be allowed for […]
Colorado’s Medicaid Expansion Plans Make Sense
Governor Hickenlooper’s announcement last week that Colorado plans to expand Medicaid eligibility to more than 160,000 childless adults has been met with much debate from both sides of the political spectrum. The voices opposed to the expansion come mainly from an economic perspective, saying that we just can’t afford to cover more people with Medicaid. And as is usually the case, there are wildly different estimates of how much the Medicaid expansion will cost and/or save the state over the next decade: The Kaiser Family Foundation says that the move will cost Colorado $858 million over the next decade, while Governor Hickenlooper’s office says that it will save $280 million instead.
After all of the money talk from the CBO and all of the special interest groups over the last few years regarding various aspects of the ACA, I think a lot of people have become numb to the numbers. Predictions of how much any healthcare legislation will cost or save over any lont-term time horizon really depend on who is doing the study and what variables they took into consideration. And we have to bear in mind that laws and reforms and healthcare in general are not static entities; they’re constantly changing, which makes long-term financial predictions murky at best. Even if we could control for every single current variable and come up with an accurate picture of the cost and/or savings implications of the Medicaid expansion, we can’t know what additional changes might be made in the future that will increase or decrease the predicted amounts. Given that reality, as well as the dramatically different financial predictions out there, I think it’s best to assume that the actual numbers will […]
CLASS Act Officially Nixed From The ACA In Fiscal Cliff Deal
[…] CLASS wasn’t going to be financially viable, and the first try just didn’t work. But that doesn’t mean we can just forget about it and move on. One way or another, long term care costs have to be addressed relatively soon. My prediction is that a new bill will be crafted in the next couple of years to create a solution similar to CLASS but hopefully with a more solid financial groundwork. But I think lawmakers might wait until 2014 – after the ACA has been more fully implemented and health insurance coverage is more widespread than it is today – to take action.
Senator Aguilar Pushes For Universal Healthcare In Colorado
Senator Aguilar’s plan for universal healthcare in Colorado is based on a genuine need: even with current and planned state and federal healthcare reforms, there will still be a lot people in Colorado without health insurance. The CBO estimates that on a national level, we’ll have 30 million uninsured people in the US a decade from now. That’s taking into account the fact that SCOTUS struck down a provision in the ACA that would have required states to expand their Medicaid programs. States have flexibility with that now, and some will likely choose not to expand. Colorado, however, is expected to expand its Medicaid program (not surprising, given how much work the state has already done on that front). The uninsured population in Colorado hovers somewhere in the 600,000+ range, depending on how and when the samples are studied. If the ACA is expected to reduce the national uninsured population from 53 million to 30 million, and taking into account the fact that Colorado will likely be one of the states that opts for Medicaid expansion, I would say it’s reasonable to expect that the uninsured population here will be reduced by at least 50% once the ACA is fully implemented. But that still potentially leaves a few hundred thousand people – not an insignificant number by any stretch – with no health insurance. Those are the people Senator Aguilar is trying to help.
Health Insurance And Genetic Testing
[…] Is it fair to say that health insurance carriers shouldn’t be able to use genetic testing information during underwriting, but that they should have to pay for preventive healthcare that results from genetic testing? I don’t think there’s an easy answer there. It’s hard to put a price tag on health and life, and it’s difficult to say that a person who is making such a hard decision should also be faced with a potentially very large medical bill at the same time. But if we’re going to categorically state that genetic testing cannot be used to the advantage of health insurance carriers, it’s hard to turn around and say that the carriers should also be required to pay for treatment that comes about as a result of that same testing.
What do you think? As technology moves forward, I have no doubt that genetic testing will become more routine, and various preventive measures based on those tests will likely become fairly commonplace. If they become a larger part of our general healthcare process, I would say that it’s reasonable to assume they will also be covered more frequently by health insurance carriers. And as of 2014, some of the issues addressed by GINA will become moot points too, as health insurance will all be guaranteed issue. So this is a subject that might just work itself out naturally over the next decade or so. But for now, it does leave plenty of room for debate.
What Should Health Insurance Cover?
The reason we have health insurance is to protect against the things we don’t expect to happen. The things we can’t foresee. The things that would blow though most households’ life savings very quickly. Doctor visits, routine medications, even the occasional trip to urgent care – these are relatively predictable. And relatively inexpensive, compared with the cost of care for a serious illness or injury.
If health insurance did cover everything, without any additional out-of-pocket costs for the insured, health insurance premiums would go up by about as much as people currently spend on out-of-pocket costs. Health insurance carriers would have to start generating enough revenue to cover those claims, and that would translate directly into higher premiums for everyone.
I know that the comparisons between health insurance and auto or home insurance have been made many times, but I’ll bring it up again here. When you buy car insurance, you don’t expect it to cover oil changes, new tires, or even a whole new engine if your car ends up needing one. When you buy home insurance, you don’t expect it to pay for home maintenance or repairs. In both cases, we expect the insurance to cover the unexpected. We know that if we have a car or a house, they’re going to need maintenance. And we know that we’ll have to budget for those things, however much we might dislike that fact. We hope that we never have to use our car insurance or our homeowner’s insurance. The same should be true of our health insurance. It’s there in case something unforeseen and expensive occurs (and it’s useful to remember that “expensive” is a relative term… although $1000 is “expensive” as far as most family budgets, it’s a tiny fraction of the total medical bill that would be incurred in the event of a major illness or injury). When you take that view of health insurance, it becomes a more realistic product. With most policies, the money you’re paying in premiums is not intended to cover routine, minor healthcare (with the exception of preventive care). But it will cover the potentially enormous claims that could result from a serious illness or injury.
Should Dental Insurance Be Included On Health Insurance Policies?
[…] One possible solution would be for dental insurance to get wrapped in to health insurance policies, both private coverage and Medicare (the majority of seniors in Colorado have no dental insurance, because it’s not part of Medicare). If dental insurance were absorbed into health policies, the premium increases might not be significant. Maternity coverage is a good example of how this could work. In the past, maternity coverage was only available on a few individual health insurance policies in Colorado, as a separate rider that had to be added to the basic coverage. The cost for this rider was prohibitive, because the only people who were adding it were the ones who were planning to use it. But for almost two years now, all new individual policies in Colorado have included maternity coverage, and premiums have definitely not increased by as much as maternity riders used to cost (premiums have gone up, as they had done for years prior to the maternity mandate, but there are many factors involved). If dental coverage were included in health insurance policies, the administrative overhead for these plans could be rolled in with the administration of the health plans, and there would be more people who had coverage and weren’t using it often – their premiums could offset the cost of dental care for people with significant claims. […]
Downsides To Raising The Medicare Eligibility Age
[…] The wealthiest older Americans can probably easily wait until 67 for Medicare. In 2014, individual health insurance will be guaranteed issue, and if paying the premiums is not a problem, that’s a viable alternative for some people. But most Americans are not wealthy enough for those premiums to be easily affordable, even with premium subsidies. More than a few 65 and 66 year olds would likely opt to go uninsured until they reached the new Medicare age, and that brings it’s own host of problems – for the individuals and for taxpayers, hospitals and the entire healthcare system. For people struggling to make ends meet, an extra two years of either being uninsured or stretching to pay health insurance premiums could be a very big deal indeed. And as Maggie points out, it doesn’t even end up saving money.
The proposal to raise Medicare eligibility to 67 is short-sighted and based on the premise that Medicare is an “entitlement” (what about the fact that recipients have been paying into it for decades, to cover the cost of previous retirees’ care?). I suppose it makes sense – at first glance – that we can reduce the amount spent by Medicare if we make people wait an extra two years to enroll. But the practical realities would be a different story: people putting off medical care until age 67 (at which point illnesses might be more progressed and more expensive to treat), people going uninsured, higher premiums within the Medicare system without the younger members enrolled, higher costs borne by employers who cover the cost of healthcare for workers and retirees, and the list goes on. […]
Health Insurance Premiums Mirror Healthcare Costs
[…] Colorado has taken a much more proactive and transparent position in terms of the rate review process, and we’ve written about it several times. Although rate increases on health insurance policies are frustrating when they continue to far outpace inflation, they’re being driven largely by the increases in the cost of healthcare. But most of us are very insulated from the cost of our healthcare. Since the bills go to our health insurance carriers, many people don’t really know how much it costs to have any sort of significant medical treatment. We know how much our health insurance costs though, and when the price goes up, we feel it. Even though the price increase is directly linked to the increases in healthcare spending, we’re much more likely to focus on the health insurance premiums, since those are the bills we pay ourselves (this is especially true for people who buy their own individual health insurance, without assistance from an employer). […]
Rocky Mountain Health Plans 2013 Rate Increase Announced
Rocky Mountain Health Plans announces the 2013 new business rate increase for the “SOLO” individual/family health insurance plans in Colorado is 18%. As with all carriers, for existing clients on open plans, rate changes may be different due to age attainment and trend. Carriers may adjust rates differently for closed plans effective January 1, 2013.
RMHP posted the disclosure of the increase for new and renewing business on healthcare.gov.
For clients who pay monthly:
- January renewals were mailed Friday, November 30, 2012.
- February renewals will be mailed the end of December.
- March renewals will be mailed the end of January.
No 2013 Rate Increases for Cigna or Anthem Blue Cross of Colorado
Both Cigna and Anthem Blue Cross of Colorado report no rate increases on new business in Colorado. However, for existing clients on open plans, rates may change due to age attainment and trend. Carriers may adjust rates for closed plans effective January 1, 2013.
How the Affordable Care Act Affects You
For the first couple years after the Affordable Care Act was signed into law, everything seemed to be a bit up in the air. There was almost constant bickering about the subtle nuances of the legislation, along with uncertainty from both sides of the political spectrum insofar as whether or not the law would stand the test of time. The Supreme Court had to weigh in, and we also had a major election cycle midway between the signing of the law and the enactment of many of its main provisions.
Most of that has settled down now. SCOTUS upheld the law. And there was no election upheaval in Congress to tilt the legislative body towards a crowd that would be likely to repeal it. States – like Colorado – that had been working towards setting up a health benefits exchange can continue to do so without as much worry that their work might be in vain (there had been some concern that the law would be tossed after states had invested a lot of time and money in the exchange-creation process). We are just over a year out now from January 2014, when many of the major provisions of the ACA will go into effect; it seems relatively certain at this point that the ACA will continue to move forward now that some of the potential roadblocks are in the rearview mirror.
Several provisions of the Affordable Care Act – ACA have already been implemented over the past two years: Young adults can remain on their parents’ health insurance policy until […]
Individual Health Insurance After Donating A Kidney
This recent AARP article caught my attention last week. My father lost his kidneys in 2001 as a result of Wegener’s Granulomatosis, a rare autoimmune disease. In August, he was the recipient of a kidney generously donated by the family of a young man who had passed away. And this fall, for the first time in 11 years, he’s been able to go about his life without being tethered to a dialysis machine every evening. So I’m drawn to stories about kidney transplants, living donors, or families who choose to donate a deceased loved ones organs.
To sum it up, Radburn Royer is a healthy 57 year old who donated a kidney to his daughter four year ago, after her own had failed as a result of lupus. Prior to donating a kidney, Royer was covered by Blue Cross Blue Shield of Minn. It’s unclear what his health insurance status was in the interim, but last year he reapplied for coverage with them and was turned down. He’s appealed several times, but for now he’s covered by his state’s high risk pool (he has to pay $130 more per month for his coverage and has a higher deductible, both of which are common in high risk pools).
Individual health insurance in Colorado is underwritten just as it is in Minn., but underwriting guidelines usually vary from one state to another and from one carrier to another. So we contacted three of the top individual health insurance carriers in Colorado to see how they would underwrite an applicant who had previously donated a kidney. Cigna, Humana and Anthem Blue Cross Blue Shield all said that as long as the donor had been released from medical care and had normal blood pressure and blood lab results, the most likely underwriting outcome would be acceptance with a standard rate.
At first glance, this seems to be at odds with the situation experienced by Royer, but maybe it’s not. The AARP article notes that Royer underwent […]
[…] In the context of kidney donation, it’s important that potential donors not be inadvertently scared off by AARP’s article. Kidney donors are heroes – anyone who had received a transplant will attest to that fact – and they save lives. The study that I linked to above followed donors for 20 – 37 years after their transplants. While some donors did end up having kidney problems, the majority had normal kidney function 20 – 37 years out from surgery, and would likely not have a problem obtaining individual health insurance, even prior to it being guaranteed issue in 2014. Most people who are healthy enough to be accepted as a donor will continue to be healthy after they donate a kidney.
I wish my health insurance _____________?
I understand the trade off we got when we switched to a really inexpensive high deductible plan when even our high deductible HSA qualified plan was too rich and expensive. So I wish my health insurance had a monthly credit card billing option. Our current health insurance company, Anthem Blue Cross of Colorado used to have it, like most health insurance companies did. But then, like most other companies also did, they stopped offering that as an option about a year ago.
What would you change about your health insurance company or plan? It could be the coverage, billing, customer service, anything…
2012 Obamacare Premium Rebates (Infographic)
Did you receive a health insurance premium rebate this year? If so, how much was it? We created a simple visualization of how the PPACA (Obamacare) health insurance premium rebates break down between the individual/family, small group and large group markets and how Colorado’s rebates compared to the national average.
")